

Behind the JCO Editorial: The Full Trial Record
The survivor trial architecture, the formulation evidence, and the broader health data that the editorial had to compress. This is the full evidentiary map.

Don Dizon, MD, at Tufts Medicine and I recently published an editorial in the Journal of Clinical Oncology arguing that menopausal hormone therapy (MHT) after breast cancer warrants individualized risk-benefit discussion, not blanket prohibition. An editorial makes the argument concisely. What it cannot do is show its work.
This piece shows the work. It is designed for clinicians and medically sophisticated readers who want the trial-level detail underneath the public argument: what the survivor studies actually tested, why they diverged, what evidence has accumulated since, and what tools make individualized counseling practical rather than aspirational. This piece is for paid subscribers; the patient-facing post is free and shareable.
1. Reading the Survivor Trials: What the Literature Actually Tested
Much of the confidence behind blanket contraindications comes from treating the survivor literature as a single verdict. It is not. These trials tested different interventions, in differently managed populations, with different durations and methodological constraints.
HABITS (1997–2003)
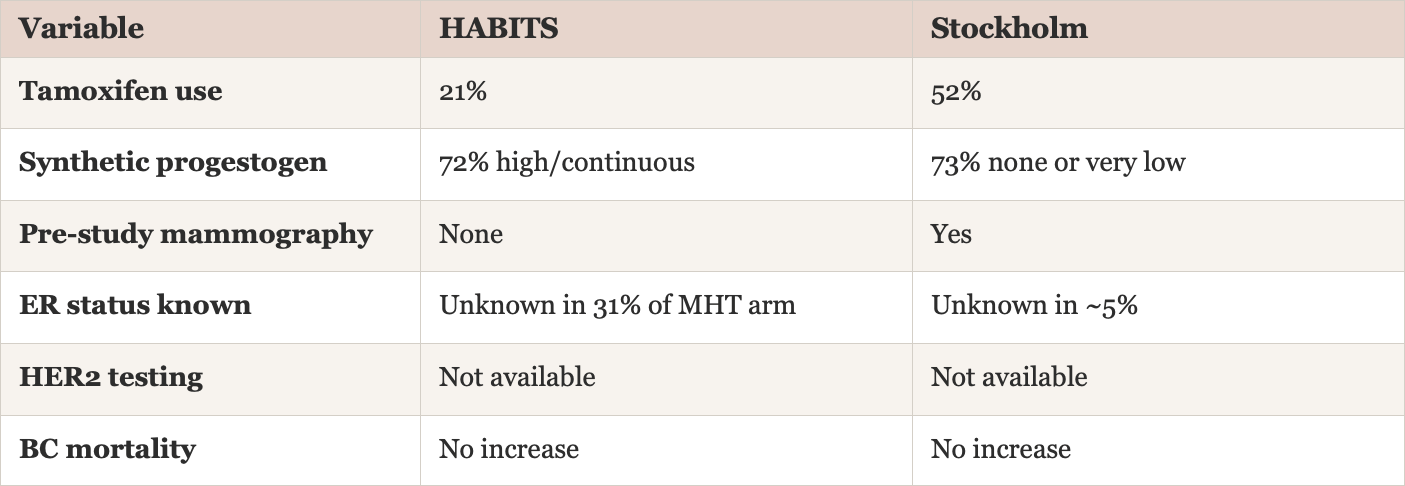
434 Scandinavian women with stage 0–II breast cancer (ER+ or ER−), randomized to open-label clinician’s-choice systemic MHT or management without MHT. Follow-up available for 345 (174 MHT, 171 control). 21% received estradiol alone. 72% with a uterus received estrogen plus synthetic progestogen (mostly norethindrone acetate, NETA), 46% continuous, 26% cyclic. Only 21% used concomitant tamoxifen.
At 2.1 years: 26 events MHT vs. 7 control (HR 3.5; 95% CI 1.5–8.1). Signal specific to HR-positive disease.
At 4 years: 39 events vs. 17 (HR 2.4; 95% CI 1.3–4.2). No difference in breast cancer mortality at either timepoint.
Limitations: Early termination; ER status unknown in 31% of MHT arm; no pre-study mammography; no HER2 testing (unavailable in that era); high-dose continuous synthetic progestogen in the majority; investigators could not discriminate impact by preparation type due to small numbers.
Stockholm (1997–2003)
378 women with stage 0–III breast cancer (ER+ or ER−), randomized to MHT (188) or control (190). 52% on concomitant tamoxifen. Designed to minimize synthetic progestogen exposure: 23% estradiol alone, 50% estradiol plus spaced MPA every 84 days, 22% estradiol plus monthly cyclic MPA. Net: 73% had no or very low synthetic progestogen exposure.
At 4.1 years: 11 events MHT vs. 13 control (HR 0.82; 95% CI 0.35–1.9). No significant increase.
At 10.8 years: 60 events MHT vs. 48 control (HR 1.3; 95% CI 0.9–1.9). Contralateral cancers slightly increased (14 vs. 4), half with different histology, suggesting second primaries. No difference in overall or breast cancer mortality.
Stockholm was stopped in December 2003 based on the HABITS safety signal, not its own data. Its authors concluded that MHT should not be forbidden in symptomatic breast cancer survivors.
MD Anderson (Prospective Cohort)
319 women enrolled; 222 refused randomization. Of 77 who agreed, 34 were randomized to CEE, 43 to no CEE. Another 22 chose CEE. None used progestogens. In the 56 women who took CEE (median follow-up 5.9 years), recurrence was not elevated (HR 0.72; 95% CI 0.47–1.10): 2 of 56 (3.6%) vs. 33 of 243 (13.5%). This trial is frequently grouped with RCTs; it should be understood as a prospective cohort.
LIBERATE: The Tibolone Distortion
LIBERATE tested tibolone—a selective tissue estrogenic activity regulator (STEAR)—vs. placebo in 3,184 women with breast cancer (71% ER+). Tibolone is not estradiol. It is not progesterone. It has a distinct pharmacological profile, and the US FDA rejected it for safety concerns.
Result: Increased recurrence (HR 1.40; 95% CI 1.14–1.70), primarily ER+ (HR 1.56). Highest risk in women on aromatase inhibitors at enrollment (HR 2.42; 95% CI 1.01–5.79). Not significant in ER-negative women (HR 1.15).
This matters because of how LIBERATE enters the meta-analytic literature. The Poggio 2022 meta-analysis pooled HABITS, Stockholm, LIBERATE, and MD Anderson as though all tested the same exposure. LIBERATE drives the aggregate recurrence signal. The Coronado 2024 analysis (Spanish Menopause Society) separated LIBERATE and found: no significant recurrence increase with actual MHT (RR 0.85; 95% CI 0.54–1.33), no mortality impact, and in estrogen-vs.-no-estrogen comparisons regardless of study design, no increased recurrence risk.
Any meta-analysis that includes LIBERATE without flagging that tibolone is pharmacologically distinct from estradiol/progesterone-based MHT conflates a different drug with the class under discussion.
Contemporary Treatment Era
All four survivor trials predate contemporary treatment: widespread aromatase inhibitor use, risk-based chemotherapy and ovarian suppression, HER2 testing and targeted therapies, immunotherapy for triple-negative tumors, and modern tumor profiling. These advances significantly improve baseline outcomes and change the risk calculus. The older trials tested different drugs, in a different treatment era, in women whose cancers were not characterized by today’s standards.
2. What Explains the Divergence
The HABITS/Stockholm split is routinely presented as ambiguity. It is better understood as a formulation signal hiding in plain sight. The trials did not test the same drugs in the same way. The variable that most clearly tracks the divergence is progestogen exposure, and the pharmacology underneath it.
The Progestogen Variable
