

The Category Error That Is Costing Women Their Health
When your doctor says “no hormones,” they are collapsing three different stories into one word. The differences change everything.

In the last post, I wrote about why the blanket prohibition on hormone therapy after breast cancer doesn’t survive contact with the evidence. Today I want to go one layer deeper, into the mistake underneath the mistake.
The deepest problem in this conversation is not that doctors are cautious. Caution is reasonable when uncertainty is real. The problem is that the word “hormones” has been allowed to do the work of an entire category, as though it names one exposure with one biology and one risk profile. It does not.
In 2002, the Women’s Health Initiative was stopped early. The headlines were terrifying: hormones increase breast cancer risk. Millions of women threw their prescriptions in the trash. But women did not stop taking hormones because the science showed harms. They stopped because the message they heard was simplified and did not apply to most women taking menopausal hormone therapies.
The study didn’t test “hormone therapy” as a whole. It tested two specific, older, synthetic hormones: alone or in combination. And for two decades since, medicine has committed what I call a category error: treating every type of hormone, every route of delivery, every dose as though they all carry the same risk. That confounding of the evidence has left millions of women suffering unnecessarily.
When a woman hears “no hormone therapy,” she is hearing a single prohibition that collapses at least three separate questions: Which estrogen? Which progestogen? And what about testosterone, the hormone no one mentions and most clinicians have no training on at all? Until those questions are separated, neither the doctor nor the patient is actually talking about the evidence. They are talking past it.
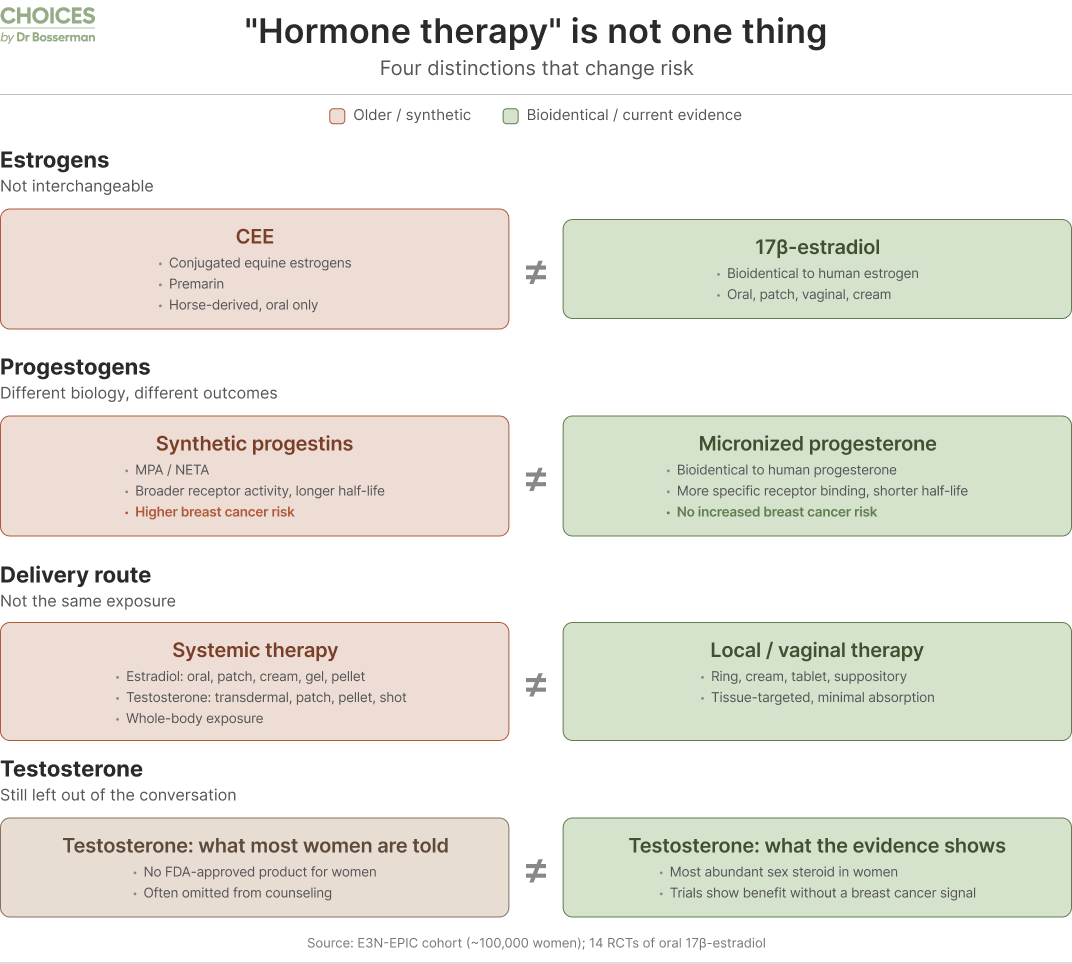
1. The Estrogens: CEE Is Not Estradiol
The fear that “estrogen causes breast cancer” was shaped by the WHI study of two synthetic drugs: conjugated equine estrogen, CEE with the synthetic progestogen, medroxyprogesterone Acetate (MPA) and not when they used CEE alone. But here is something most women are never told: the WHI did not use the kind of bio-identical estrogens or natural progesterone that most doctors prescribe today.
The WHI used only conjugated equine estrogens — CEE, a complex mixture from pregnant horses with at least ten different estrogens used by horses but not all by women, sold as Premarin. That is not the same molecule as 17β-estradiol, which is the estrogen women’s bodies make, which is bioidentical — meaning it is chemically identical to the estrogen the ovaries produce before menopause. They behave differently in your body, and the data reflects that difference. Neither oral CEE nor oral bioidentical 17 beta-estradiol increases breast cancer risks but they have very different effects on our blood vessels and blood clotting risks.
Across fourteen randomized trials of oral 17β-estradiol — the bioidentical form — there was no increased risk of venous blood clots (VTE) or breast cancer above baseline population rates. The best available data suggests women on oral estradiol, alone or with micronized progesterone, have a VTE risk of roughly 6 per 10,000 women per year, which is the same as the normal background rate of 6-12 per 10,000 women per year aged 50 to 59.
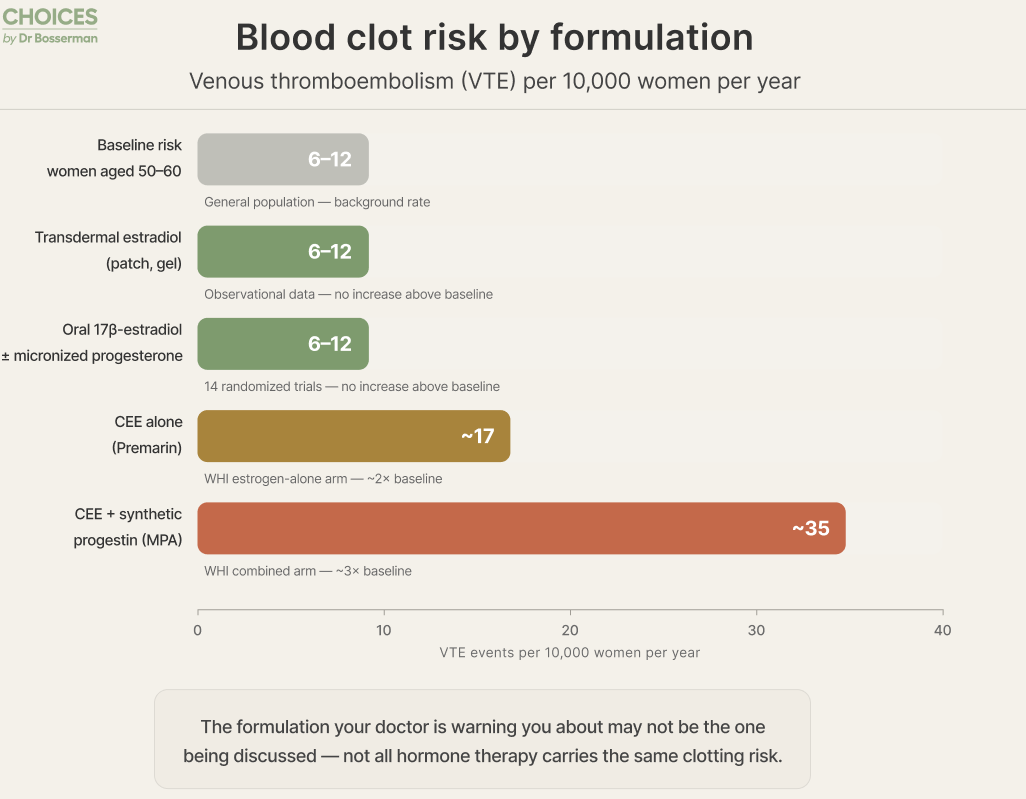
Compare that to CEE, the horse-derived 10 estrogens from the WHI where the WHI study showed an increased VTE risk of about 17 per 10,000 women per year when used alone, rising to approximately 35 per 10,000 when combined with the synthetic progestin, MPA.
Those are not the same numbers. They are not the same molecule. They should not be discussed as though they are the same thing. Yet in most clinical conversations, they still are.
2. The Progestogen: Synthetic vs. Bioidentical
If the estrogen confusion has been costly, the progesterone confusion has been catastrophic.
There are two fundamentally different substances that get called “progesterone” in medical conversations, and the failure to distinguish them has distorted an entire generation of clinical practice.
Micronized progesterone — the bioidentical form, structurally identical to what your body produces — has a shorter half-life and binds specifically to the progesterone receptor and is primarily antiproliferative. It does not significantly cross-react with the proliferative glucocorticoid, androgenic, or mineralocorticoid receptors.
Synthetic progestins — including medroxyprogesterone acetate (MPA, sold as Provera) and norethisterone acetate (NETA), are structurally different molecules. They last much longer in the bloodstream and bind to multiple receptor types, producing a broader proliferative set of biological effects.
These differences explain the very different impacts on breast cancer risks which are not theoretical distinctions. The E3N-EPIC cohort study in women without breast cancer, followed nearly 100,000 French women, found that estrogen combined with synthetic progestogens increased breast cancer risks 40% as shown by the scientific term: hazard ratio of 1.4. Estrogen combined with micronized progesterone did not — hazard ratio 0.9. Estrogen alone, whether CEE or estradiol, showed no increases either.
Read those numbers again. One combination with synthetic progestogens raised risk. The trials without synthetic progestogens did not. The difference was the progestogen.
This likely explains one of the most important puzzles in the survivor literature when older hormone therapy combinations were used in two major studies in women with breast cancer. The HABITS trial — the study most often cited as proof that hormone therapy is dangerous after breast cancer — used predominantly synthetic progestins, with 72% of women receiving higher-dose continuous synthetic progestogens. The Stockholm trial, which ran in parallel in women with breast cancer, found no statistically significant increase in recurrence. The Stockholm trial had 73% of women on low or no progestogen exposure and much higher rates of tamoxifen use. Neither trial showed increased breast cancer mortality.
When papers, AI summaries, and even journal editors use the word “progesterone” to mean synthetic progestins, they perpetuate a confusion that costs women access to therapies the evidence does not actually condemn. In our JCO editorial, Don Dizon and I called on journal editors to enforce rigorous terminology: progesterone should mean micronized progesterone. Progestins should mean synthetic progestins. These are not interchangeable words. They describe different molecules with different safety profiles. Natural, bio identical progesterone has not been associated with increased breast cancer risks in women or in wommen with BRCA 1 or 2 mutations who have a high risk of getting a breast cancer.
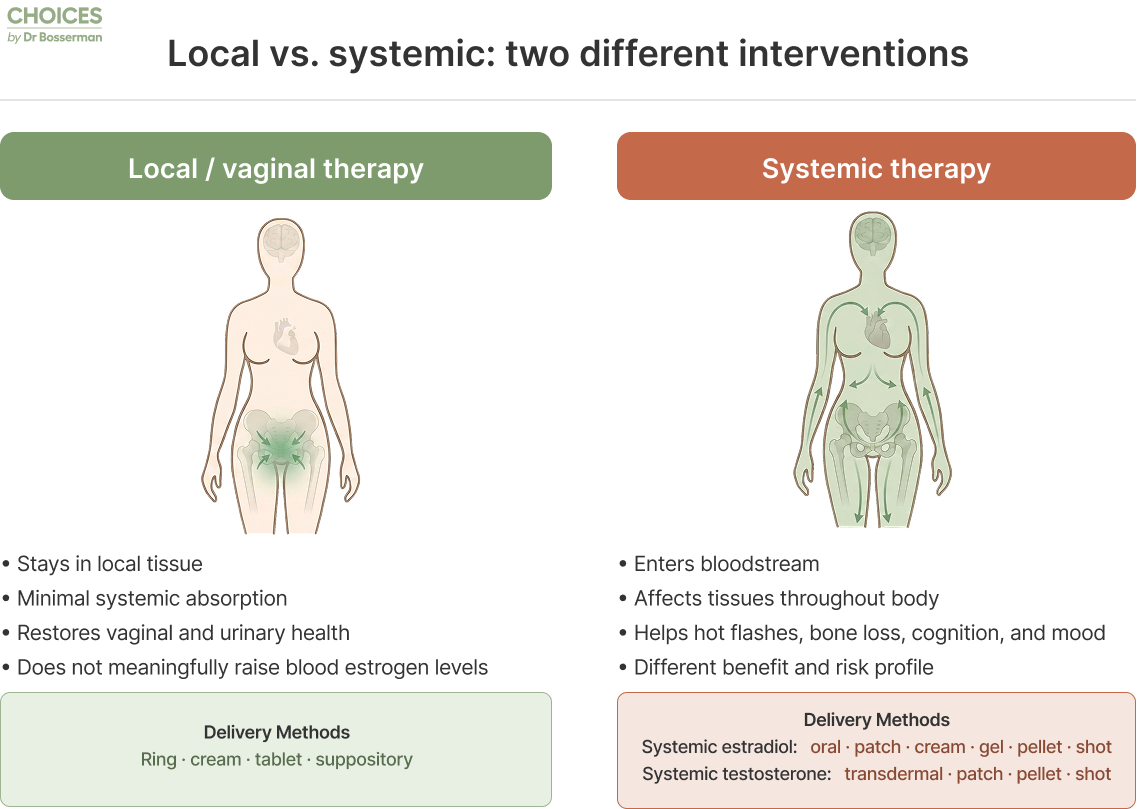
3. The Delivery: Local vs. Systemic
For many women, denial of any type of healing hormone therapies is not an abstract debate. It is about the lived reality of urinary burning, recurrent infections, vaginal dryness, itching, tissue fragility, and pain with intimacy.
Local vaginal therapy treats only the specific tissues of the vagina, vulva, and bladder. The doses are microscopic and do not raise the estradiol blood levels. And for breast cancer survivors specifically, a 2025 systematic review and meta-analysis spanning more than 50,000 women-years — including women on aromatase inhibitors — found no significant increase in breast cancer recurrence or mortality. Local, low dose, bio identical estradiol in a low dose ring, a vaginal tablet or vaginal suppository or a cream you can rub a pea to grape size amount on the outsid of the vagina, the vaginal opening and the inside are all safe to use daily for 2 weeks then 2-5 times per week as needed to heal and keep the vulva, vaginal opening and vagina walls healed, elastic and healthy.
Systemic therapy (oral pills, pellets or skin gel or skin patches) sends estradiol or testosterone through your bloodstream to treat whole body symptoms of hormone losses including hot flashes, protection of bone loss, local vulva, vaginal opening and internal vaginal sympotms along with helping protect the blood vessels, heart, brain, joints and well being along with other whole-body effects of menopausal hormone losses or deprivation.
Many women are told they cannot use even low dose vaginal estradiol. The evidence does not support that and it is important to heal as untreated, vulvovaginal breakdown and symptoms progress and cause preventable recurrent urinary infections and whole body urinary caused infections.
4. The Hormone No One Mentions: Testosterone
Here is something that surprises most women: testosterone is actually the most abundant sex steroid in women’s bodies from age six throughout life. Women have less testosterone than men — roughly one-tenth the concentration — but they have more testosterone than estradiol at every stage of life, as do men.
This is not a male hormone that women happen to have. It is a foundational hormone for women’s physiology that impacts energy, sexual desire, muscle health, emotional well-being, bone density, and cognition. And yet there is no FDA-approved testosterone product for women in the United States… yet!
Four randomized trials of more local, lower-dose vaginally applied testosterone in women with hormone receptor-positive breast cancer showed improvement in vulvovaginal atrophy and desire without raising serum estradiol levels. Longer-term observational data on higher, female dose whole body testosterone using pellets in breast cancer survivors showed no increase in breast cancer incidence over 10 to 15 years compared to WHI placebo rates nor in women without breast cancer.
The evidence base is not as deep as we need it to be. But the safety signal so far is reassuring, and the clinical reality — that millions of women are suffering from symptoms that testosterone can address — yet no studies show increased breast cancer risks, deserves more than silence.
5. Your Health Is Not Only About Breast Cancer
There is one more piece of the evidence that I want women to understand, because it reframes the entire conversation about risk.
When your oncologist discusses hormone therapy, the frame is almost always breast cancer recurrence. But breast cancer is not the only serious health risk women face after menopause, and the majority of women with breast cancer in the US have early, curable disease after therapies. Cardiovascular disease kills more women with breast cancer than breast cancer does. Bone fractures carry a significant mortality risk. Cognitive decline is one of the most feared outcomes of aging. And none of these are addressed by the blanket prohibition against using whole body hormone therapies with estradiol, testosterone, and natural progesterone.
The evidence, while not sufficient to justify prescribing hormones solely for prevention of these conditions, suggests that the timing, formulation, and context of hormone therapy matter for improving these outcomes too.
The Danish Osteoporosis Prevention Study (DOPS) randomized roughly 1,000 women, average age 50, without breast cancer, to ten years of 2 mg per day of oral estradiol. At sixteen years of follow-up, the hormone therapy group showed a 52% reduction in the combined endpoint of death, heart failure, or heart attack. Major cardiovascular reductions persisted even years after therapy was stopped. And, there was no increase in breast cancer, blood clots, stroke, or dementia.
The ELITE trial in postmenopausal women without breast cancer showed that oral estradiol started within six years of menopause slowed the progression of arterial thickening — a validated marker of atherosclerosis risk — which is the cause of heart attacks and strokes, compared to the same therapy started later.
The KEEPS trial in post menopausal women without breast cancer, showed that hormone therapy started within three years of menopause halted the rapid bone loss that normally occurs in those early years, reducing hip and vertebral fractures by 20 to 40%.
And four large observational studies — Cache County, MIRAGE, Baltimore Longitudinal, and Kaiser Permanente —reported that early use of estrogen therapy in menopasual women without breast cancer may significantly delay or reduce the risk of Alzheimer’s disease, compared to women who never used it or who started it much later. NO other therapies have been shown to consistently reduce Alzheimer’s and dementia risks.
None of this means every woman should take hormones for her heart or her brain. But it means that when a woman is told “no hormones” after breast cancer, the person saying it should be weighing these competing risks — not just the one they were trained to focus on.
Five Questions for Your Next Appointment
I am not asking you to override your oncologist. I am asking you to insist on precision.
1. “Which hormone are we talking about?” Estradiol or conjugated equine estrogens? Micronized progesterone or synthetic progestins?
2. “Which route — local or systemic?” A low-dose vaginal cream and a systemic pill are different exposures with different evidence.
3. “What is my actual recurrence risk?” Ask for the number, not a feeling. Tools like Predict Breast v3 can estimate your 5 to 15 year outlook and show how it compares to your risk of dying from other causes.
4. “Compared to what?” What are my risks from cardiovascular disease, bone fracture, cognitive decline, and years of untreated symptoms?
5. “Which studies actually apply to my situation?” Which trials used my type of cancer, my treatment era, and the specific therapy being discussed?
Ask for the numbers, not the narrative.
An honest answer may still be cautious. It may still be no. But it will be an answer that has actually engaged with the evidence, rather than a reflex inherited from a study that used different drugs in a different population, a generation ago.
You deserve an earned answer. Not a borrowed one.
In the next post, I’ll walk through what an honest, individualized conversation about hormone therapy after breast cancer should actually include, for both patients and the clinicians who want to have it.
👉 Read “Personalization, Not Prohibition” in the Journal of Clinical Oncology
Co-authored with Don S. Dizon, MD, FACP, FASCO, Tufts Medicine